Used for fistula or grafts HeRO save ® graft

HeRO (hemodialysis reliable outflow) graft is an entirely subcutaneous solution, used to save by around central vein stenosis fistula or AV graft loss.
The benefits of saving
- Access site protection: save the loss of AVF or AVG to avoid using the new pathways and bridging catheter1
- Removable and replaceable: unlike stents, HeRO graft vein outflow components can be removed and replaced when necessary
Identify AVF or AVG save candidates
If your answer is yes to any of the following problem, please consider your referral patients for central venous imaging in the evaluation of central vein stenosis on both sides.
- Patients with loss of AVF or AVG?
- Measured is less than 1.4 Kt/V?
- Flow rate > 20% drop?
- Patients have arm swelling and/or collateral venous expansion?
seize"The window of opportunity=
Collaboration of multi-disciplinary team (IDT) for before AVF or AVG venous outflow obstruction to catch the "window of opportunity" for AVF placement is very important for the HeRO graft or AVG save (figure 1).2

Figure 1: close to narrow fistula occlusion of the venous outflow.

Figure 2: the center vein stenosis and collateral vein of patients.
Program overview
Usually, the HeRO a short ePTFE graft part with arteriovenous fistula (AVF) and arteriovenous graft (AVG).
If the existing AVF mature or merge the AVG, one advantage of this approach can be immediately for intubation pathway.This eliminates the need for bridging catheter.Don't need to bridge the benefits of dialysis catheter is to avoid the risk of infection.

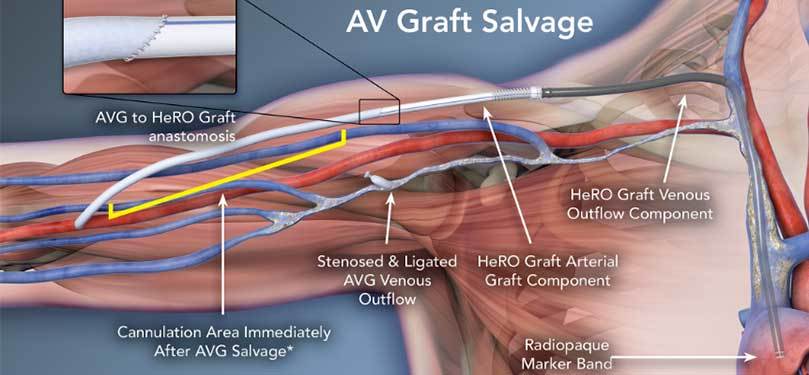
* if the AVF mature or merge the AVG.According to your agreement for the dialysis of care and intubation.
Clinical data
The following clinical cases involving in AVF or AVG save for the purpose of HeRO graft.
| The author and publication | Important data points | |
| AVF save | Chen, G, etc.EJVES Extra. 2011;22 (4) : e37-39. |
Patients with functional AVF arm edema by central venous system occlusion case report, the patient endovascular treatment of repeated twice within two years (including stenting) is invalid. Arm swelling resolved, connect to the HeRO grafts can be used immediately after the AVF. Six months after holding function is normal, need not intervene again. |
Bowers V, etc.VASA.2010 Las Vegas, NV. J Vasc Access, 2010;11 (S2) : S26-27. |
Two patients received HeRO Graft to save caused by central vein stenosis of AVF failure case report. HeRO Graft implants to avoid the use of bridge the needs of the catheter. Also emphasized the value of teamwork, thanks to IDT method and timely communication, so as to save the AVF. |
|
| AVG and AVF save | Gage S and others.Ann Vasc Surg 2011;25 (3) : 387. E1-5. |
Two arms by central venous system occlusion oedema patient case report: a functional AVF, a functional AVG. Two patients has been accepted by a variety of interventions, including angioplasty and stent implantation, but the recurrence of symptoms. Rather than give up functional vascular access, HeRO implanted grafts, solved the patient's arm edema and save the path. HeRO Graft twenty-one (21) months has continued. |
Allen et al., B.J Vasc Surg 2012;56 (4) : 1127-1129. |
Two case study describes the use of HeRO Graft save because of subclavian vein occlusion and failure the failure of the subclavian vein recanalization AVG and AVF. AVG or recycling of AVF can be used in the second day of dialysis, flow rate of 420-450 - ml/min. The patient's HeRO Grafts in publishing has continued to play a role of fourteen (14) months (AVG rescue patients) and five (5) months (AVF rescue patients). HeRO Graft solved a patient arm edema caused by central venous occlusive disease and pain. |
reference
- Gage S and others.Ann Vasc Surg, 2011.
- France and others.ASDIN;2010 Orlando, FL.